October 14, 2019 - NPR
Selena Simmons-Duffin
The very day President Trump was sworn in — Jan. 20, 2017 — he signed an executive order instructing administration officials "to waive, defer, grant exemptions from, or delay" implementing parts of the Affordable Care Act, while Congress got ready to repeal and replace Barack Obama's signature health law.
Months later, repeal and replace didn't work, after the late Arizona Sen. John McCain's dramatic thumbs down on a crucial vote (Trump still frequently mentions this moment in his speeches and rallies, including in his recent speech on Medicare).
After that, the president and his administration shifted to a piecemeal approach, as they tried to take apart the ACA. "ObamaCare is a broken mess," the president tweeted in the fall of 2017, after repeal in Congress had failed. "Piece by piece, we will now begin the process of giving America the great HealthCare it deserves!"
Two years later, what has his administration done to change the ACA, and who's been affected? Below are five of the biggest changes to the federal health law under President Trump.
1. Individual mandate eliminated
What is it? The individual mandate is the requirement that all U.S. residents either have health insurance or pay a penalty. The mandate was intended to help keep the premiums for ACA policies low by ensuring that more healthy people entered the health insurance market.
What changed? The 2017 Republican-backed tax overhaul legislation reduced the penalty for not having insurance to zero.
What does the administration say? "We eliminated Obamacare's horrible, horrible, very expensive and very unfair, unpopular individual mandate. A total disaster. That was a big penalty. That was a big thing. Where you paid a lot of money for the privilege [...] of having no healthcare." — President Trump, The Villages, Florida, Oct. 3, 2019
What's the impact? First of all, getting rid of the penalty for skipping insurance opened a new avenue of attack against the entire ACA in the courts, via the Texas v. Azar lawsuit. Back in 2012, the ACA had been upheld as constitutional by the U.S. Supreme Court, because the penalty was essentially a tax, and Congress is allowed to create a new tax. Last December, though, a federal judge in Texas ruled that now that the penalty is zero dollars, it's a command, not a tax, and is therefore unconstitutional. He also reasoned that it cannot be cut off from the rest of the law, so he judged the whole law to be unconstitutional. A decision from the appeals court is expected any day now.
Eliminating the penalty also caused insurance premiums to rise, says Sabrina Corlette, director of the Center on Health Insurance Reforms at Georgetown University. "Insurance companies were getting very strong signals from the Trump administration that even if the ACA wasn't repealed, the Trump administration probably was not going to enforce the individual mandate," she says. Insurance companies figured that without a financial penalty, healthy people would opt not to buy insurance, and the pool of those that remained would be smaller and sicker.
So, even though the zero-dollar-penalty didn't actually go into effect until 2019, Corlette says, "insurance companies — in anticipation of the individual mandate going away and in anticipation that consumers would believe that the individual mandate was no longer going to be enforced — priced for that for 2018." According to the Kaiser Family Foundation, premiums went up about 32%, on average, for ACA "silver plans" that went into effect in early 2018, although most people received subsidies to off-set those premium hikes.
2. States allowed to add "work requirements" to Medicaid
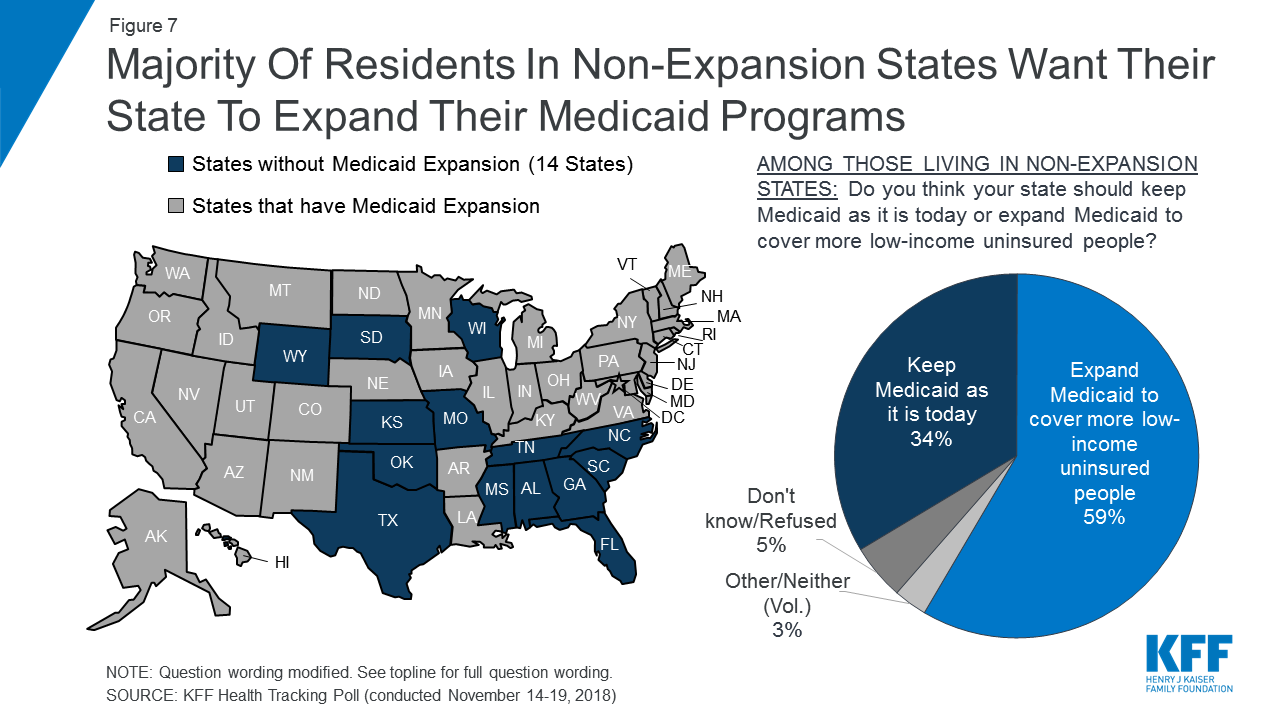
What is it? Medicaid expansion was a key part of the ACA. The federal government helped pay for states (that chose to) to expand Medicaid eligibility beyond families to include all low-income adults; and to raise the income threshold, so that more people would be eligible. So far, 37 states and D.C. have opted to expand Medicaid.
What changed? Under Trump, if they get approval from the federal government, states can now require Medicaid beneficiaries to prove with documentation that they either work or go to school.
What does the administration say? "When you consider that, less than five years ago, Medicaid was expanded to nearly 15 million new working-age adults, it's fair that states want to add community engagement requirements for those with the ability to meet them. It's easier to give someone a card; it's much harder to build a ladder to help people climb their way out of poverty. But even though it is harder, it's the right thing to do." — Seema Verma, administrator of the Centers for Medicare and Medicaid Services, Washington, D.C., Sept. 27, 2018
What's the impact? Even though HealthCare.gov and the state insurance exchanges get a lot of attention, the majority of people who gained health care coverage after the passage of the ACA — 12.7 million people — actually got their coverage by being newly able to enroll in Medicaid.
Medicaid expansion has proven to be quite popular. And in the 2018 election, three more red states — Idaho, Nebaska, and Utah — voted to join in. Right now, 18 states have applied to the federal government to implement work requirements; but most such programs haven't yet gone into effect.
"The one work requirement program that's actually gone into effect is in Arkansas," says Nicholas Bagley, professor of law at the University of Michigan and a close follower of the ACA. "We now have good data indicating that tens of thousands of people were kicked off of Medicaid, not because they were ineligible under the work requirement program, but because they had trouble actually following through on the reporting requirements — dealing with websites, trying to figure out how to report hours effectively, and all the rest."
If more states are able to implement work requirements, Bagley says, that could lead "to the loss of coverage for tens of thousands — or even hundreds of thousands — of people."
CMS administrator Verma has pushed back on the idea that these requirements are "some subversive attempt to just kick people off of Medicaid." Instead, she says, "their aim is to put beneficiaries in control with the right incentives to live healthier, independent lives."
Work requirements in Arkansas and Kentucky were put on hold by a federal judge in March, and those cases are on appeal. The issue is likely headed to the Supreme Court.
3. Cost-sharing reduction subsidies to insurers have ended.
What is it? Payments from the federal government to insurers to motivate them to stay in the ACA insurance exchanges and help keep premiums down.
What changed? The Trump administration suddenly stopped paying these subsides in 2017.
What does the administration say? "I knocked out the hundreds of millions of dollars a month being paid back to the insurance companies by politicians. [...] This is money that goes to the insurance companies to line their pockets, to raise up their stock prices. And they've had a record run. They've had an incredible run, and it's not appropriate." — President Trump, the White House, Oct 17, 2017
What's the impact? This change had a strange and unexpected impact on the new insurance markets set up by the ACA. Insurers were in a bind: They had to offer subsidies to low-income people applying for insurance, but the federal government was no longer reimbursing them.
"The first thinking [was], 'Oh gosh, that's going to cause premiums to go up, and it's going to hurt the marketplace,' " says Christine Eibner, who tracks the ACA at the nonpartisan RAND corporation. "What ended up happening is, insurers, by and large, addressed this by increasing the price of the silver plan on the health insurance exchanges."
This pricing strategy was nicknamed "silver loading." Because the silver plan is the one used to calculate tax credits, the Trump administration still ended up paying to subsidize people's premiums, but in a different way. In fact, "it has probably led to an increase in federal spending" to help people afford marketplace premiums, Eibner says.
"Where the real damage has been done is for folks who aren't eligible for subsidies — who are making just a little bit too much for those subsidies," adds Corlette. "They really are priced out of comprehensive ACA-compliant insurance."
4. Access to short-term "skinny" plans has been expanded
What is it? The ACA initially established rules that health plans sold on HealthCare.gov and state exchanges had to cover people with pre-existing conditions and had to provide certain "essential benefits." President Obama limited any short-term insurance policies that did not provide those benefits to a maximum duration of three months. (The original idea of these policies is that they can serve as a helpful bridge for people between school and a job, for example.)
What changed? The Trump administration issued a rule last year that allowed these short-term plans to last 364 days and to be renewable for three years.
What does the administration say? "We took swift action to open short-term health plans and association health plans to millions and millions of Americans. Many of these options are already reducing the cost of health insurance premiums by up to 60% and, really, more than that." President Trump, The White House, June 14, 2019
What's the impact? The new rule went into effect last October, though availability of these short-term or "skinny" plans varies depending on where you live — some states have passed their own laws that either limit or expand access to them. Some federal actuaries projected lots of people would leave ACA marketplaces to get these cheaper plans; they said that would likely increase the size of premiums paid by people who buy more comprehensive coverage on the ACA exchanges. But a recent analysis from the Kaiser Family Foundation finds that the ACA marketplaces have actually stayed pretty stable.
Still, there's another consequence of expanding access to these less comprehensive plans: "People who get these "skinny" plans aren't really fully protected in the event that they have a serious health condition and need to use their insurance," Eibner says. "They may find that it doesn't cover everything that they would have been covered for, under an ACA-compliant plan."
For instance, you might pay only $70 a month in premiums, but have a deductible that's $12,500 — so if you get really sick or get into an accident, you could be in serious financial straits.
5. Funds to facilitate HealthCare.gov sign-ups slashed.
What is it? The ACA created Navigator programs and an advertising budget to help people figure out specifics of the new federally run insurance exchanges and sign up for coverage.
What changed? In August 2017, the administration significantly cut federal funding for these programs.
What does the administration say? "It's time for the Navigator program to evolve [...] This decision reflects CMS' commitment to put federal dollars for the federally facilitated Exchanges to their most cost effective use in order to better support consumers through the enrollment process." — CMS Administrator Seema Verma, written statement, July 10, 2018
What's the impact? It's hard to document what the impact of this particular cut was on enrollment. The cuts were uneven, and some states and cities got creative to keep providing services. "We have seen erosion in overall health insurance coverage," says Corlette. "But it's hard to know whether that's the effect of the individual mandate going away, the short term plans or the reductions in marketing and outreach — it's really hard to tease out the impact of those three changes."
Overall, Nicholas Bagley says, the ACA has been "pretty resilient to everything, so far, that the Trump administration has thrown at it." Some of Trump's efforts to hobble the law have been caught up in the courts; others have not gone into effect. And, despite efforts to lure people away from the individual insurance marketplaces or to make ACA policies unaffordable, "the marketplaces have proved themselves to be remarkably resilient," Corlette says.
Abbe Gluck, director of the Solomon Center for Health Law and Policy at Yale, cautions that though the law has proven to be stronger than expected, all these actions by the Trump administration have, indeed, had an effect.
"These actions have been designed to depress enrollment — they have depressed enrollment," she says. "They have increased insurance prices." Also, the uninsurance rate for U.S. residents also went up in 2018 for the first time since before the ACA was passed.
Despite that, one of the things that have kept the marketplaces as strong as they are, Gluck notes, is that they're not all run by the federal government.
"Since the Affordable Care Act is implemented half by state governments — mostly blue states — those state governments have been able to resist these sabotaging efforts," Gluck says.
"They have been able to extend enrollment, and they have been able to do outreach, because they run their own insurance markets. And in those states there is already evidence that sabotage attacks have not been felt as strongly."
The piecemeal attacks on the ACA have made many people nervous about the future of their health coverage, Gluck says. "The most important theme of [Trump's] administration of the ACA has been to sow uncertainty into the market and destabilize the insurance pool," she says.
With open enrollment for 2020 health plans set to kick off in just a few weeks, Bagley wants people to know the ACA is still strong.
The federal health law "has been battered," Bagley says. "It has been bruised. But it is still very much alive."
{kind=link}